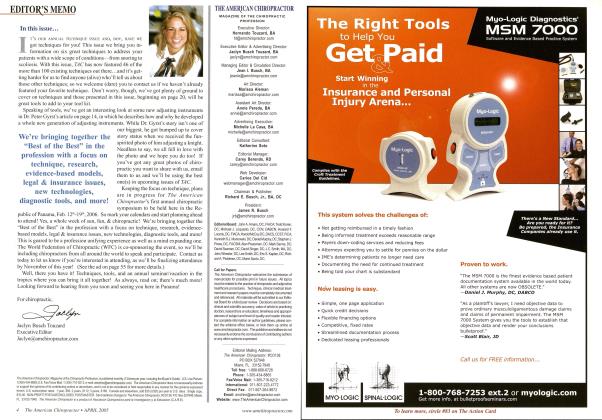
Upper airway obstruction (UAO) may be partial, in the case of snoring, or complete, in the case of obstructive sleep apnea. Narrowing of the upper airway, during sleep, causes this often serious condition, affecting millions of people worldwide. T llli UVULA AND SOFT 1'ALLF.T MAY come into partial or total contact on the back wall of the upper airway. When the contact is partial or intermittent, snoring (a loud vibration of these soft tissues) may result. The tongue may also drop posteriorly onto the back wall of the upper airway, coming into contact with the uvula and soft pallet, thus forming a tight blockage, preventing any air from entering the lungs. Respiratory effort on the part of the diaphragm and chest may cause the blockage to seal tighter. In order to breathe, the person must arouse or awaken, causing tension in the tongue and, thereby, opening the airway, allowing air to pass into the lungs. Apnea, sleep apnea or obstructive sleep apnea is defined as the cessation of breathing for 10 or more seconds while asleep.1 Traditional methods of treatment usually involve Continuous Positive Airway Pressure (CPAP) devices. Matrix Repatterning techniques were used in ten cases of long-standing, moderate to severe cases of upper airway obstruction. Matrix Repatterning Matrix Repatterning uses a manual scanning procedure to determine the location of primary structural restrictions, followed by mechanical testing to determine specific vectors of fascial tension. Treatment is generally applied manually, with light force directed into the resistance barriers. Matrix Repatterning is based on a revolutionary, new model of the underlying structure of organic tissue—the Tensegrity Matrix— which explains the complex interrelationship of all the structural components of the body. It extends the basic concept of the tissue response to injury, beyond the level of joint, muscle and ligament, to include all % structures of the body as potential sources of dysfunction.2 The tensegrity matrix model of the body, as elaborated by Stephen Levin, M.D.'and Donald Ingber, M.D., Ph.D.,4 holds that the body tissues are composed of interconnected tension icosahedra (complex triangular trusses), which inherently provide a balance between stability and mobility. This structural model explains many of the observed phenomena related to body support, movement, response to stress and trauma, as well as the effects of various therapeutic interventions. This theory has been verified by several studies in recent years. According to Ingber, a key investigator who has proven the existence of this structural model at the cellular level, "The principles of tensegrity apply at essentially every detectable size scale in the human body. At the macroscopic level, the 206 bones that constitute our skeleton are pulled up against the force of gravity and stabilized in a vertical form by the pull of tensile muscles, tendons and ligaments. In other words, in the complex tensegrity structure inside every one of us, bones are the compression struts, and muscles, tendons and ligaments are the tension-bearing members."4 Mechanism of Upper Airway Obstruction The upper airway is constructed of the hard and soft palate above, the posterior pharynx, the tongue, and the epiglottis at the level of the tracheo-esophageal junction below. There are several mechanisms of partial or complete obstruction . When the ability of the tissues to adapt or compensate becomes overwhelmed by mechanical or physiologic stress, the fas-cial system responds by altering the patterns of tension and elasticity. The tensegrity matrix explains the physiologic changes, which manifest in injured or strained tissue. The apparent fibrosis of muscle and fascia can be seen as an al- tered electro-mechanical relationship at the molecular level. The matrix is, thus, converted from a neutral, flexible form to a strained, high-energy, linearly-stiffened mode as shown in Figure 1. Obstruction may occur by approximation of several structures and tissues. This may include the soft palate retracting toward the posterior pharyngeal wall, the soft palate descending to approximate the posterior aspect of the tongue, the tongue retracting toward the posterior pharynx, or descending to approximate the epiglottis. These tissues may deviate from their functional positions within the upper airway due to a number of structural dysfunctions, including cranial vertex or occipital trauma, leading to descent and/or protraction of the cranial base, along with the maxillary portion of the roof of the upper airway. Vertex compression, in our studies, has also shown a tendency to lead to radial expansion of the upper cervical vertebrae (an intraosseous deformation), leading to loss of anterior/posterior dimension of the upper airway. Facial trauma may cause deviation of the maxilla or mandible. Hyperflexion injury of the cervico-thoracic spine may also induce an approximation of the posterior tissues toward the tongue and epiglottis. This is common in motor vehicle collisions (rear end or front end) and in falls onto the back of the head or upper back. Several other mechanisms of structural dysfunction are also currently under investigation. Assessment In cases of upper airway obstruction, a specific airway obstruction test (AOT), developed by the author, was also used to verify partial or complete obstruction. This involves placing the patient in an accentuated position of upper cervical hyperflexion or moderate extension, along with varying degrees of rotation or lateral flexion. The ease or difficulty of breathing, along with the amount of airflow turbu- lence noise, was recorded for each position. The dysfunctional structural patterns associated with snoring and sleep apnea (see above) were then evaluated using the standard Matrix Repatterning assessment. Method of Treatment A maximum of four treatments to resolve these patterns were administered over a maximum period of two months for ten patients with moderate to severe upper airway obstruction. Two of these cases were previously diagnosed with significant sleep apnea, as verified by sleep studies. Results AOT was improved significantly in 80 percent of the cases. Patients (and spouses, or sleeping partners) reported a cessation or a significant improvement in snoring in 70 percent of the cases. The two individuals, diagnosed with sleep apnea, reported they were able to sleep through the night without the assistance of a CPAP machine, on which they were previously dependant. These findings suggest that structural dysfunction may play a role in the development of upper airway obstruction and that Matrix Repatteming procedures may be beneficial in the management of these conditions. The findings suggest that a randomized controlled trial within a broader population base might be indicated.EZS Key Terms: Matrix Repatlerning, Upper Airway Obstruction (UAO), Airway Obstruction Test (AOT), Continuous Positive Airway Pressure (CPAP). References Hxar EN, Collop NA: The upper airway resistance syn drome. Chest 1W Apr: 115(4): 1127-39 The Matrix Repaltenting fragrant for Pain Relief, CSB Rolh. New Harbinger Publications. Oakland C'A, 2005. The Importance of Soft Tissues for Structural Support of the Body. SM Levin. Positional Release Therapy: As sessment tt Treatment a/ Mitseliloskelelal Dysfunc tion. K D'Ambrogio & GU Roth. Mosby-l-lscvicr. St. Louis, 1997. The Architecture of Life, OR Ingber, Scientific Ameri can. Vol. I. I'MS George li. Rolh. BSc. DC. NO. is President of The Rolh Institute, and on the Post-Gnutuale Faculty of Logan College of Chiropractic, lie can he reached by phone at 416-977-6X41. email at mfo6i-rolhmsiiuiie.com. <»■ visit w\mmlluiuiilulc.ciim. TAC's MISSION: We ore dedicated hi the continuing education & advancement of the chiropractic professional— YOU! Based on "The Architecture of Life" Scientific American 1998 Figure 1