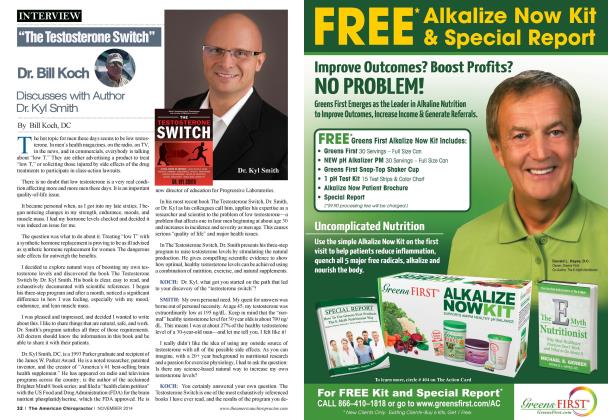
12-\ ear-old boy came into my office with severe pain at the proximal medial tibia on the left leg. He just started cross-country two weeks prior, and this pain gradually built over the two-week period to a point where he could no longer run. The coach wisely recommended the boy sec his doctor, as it looked like it was beyond the coach's ability to accurately diagnose or recommend the appropriate treatment. The young boy had played football and soccer, but this was his first year running. Running is such a repetitive motion sport that doesn't have the weight distribution diversity that football and soccer has. The stresses are constant with each and every step in running. With underlying biomechanical faults and imbalances in the lower extremities, there will be areas of increased stress, producing physiological changes (injuries) with each and every step. Maggs' Law When the loading of a tissue exceeds the capacity of that tissue, compensatory physiological changes occur. Differential Diagnosis With an injury of this nature, there are multiple degrees of injury from which the athlete can suffer. The least involved phase would be a simple shin splint, or a strain and inflammation in the medial tibial muscles. As the stresses continue, this type of injury would elevate into a stress reaction, or swelling, inflammation or edema in the bone. An x-ray in the early stages (less than 30 days) will not show signs of a stress reaction. After 30 days, it could appear on an x-ray as a subtle radiopaque line. An MRI would show edema in the bone during the early stages, and may be an appropriate test at the onset of the injury. The third phase of the injury would be a stress fracture, where the bone integrity lias been harmed. This injury- will typically occur when an athlete has ignored all signs and symptoms for a period of time (i.e. hearing "Suck it up" from the coach), and the repetitive activity continues. This degree of injury may or may not be seen on an x-ray during the early stages, but can be detected on an MRI early. The standard MRI. in most cases, will disclose the injury, but a STIR image will show the fracture more clearly. Examination Upon palpation of the area, there was extreme tenderness. There was no apparent swelling or inflammation. With the young athlete standing, it was obvious on palpation there was a gross pronation of both feet: however, the pronation was greater on the right foot. Moving up the leg. the Q angle test showed a severely increased Q angle on the right leg (uninvolvcd leg) with a moderate increased Q angle on the left leg (Fig. 1). Findings and Recommendations The x-rays were negative for fracture. This doesn't completely rule out cither a fracture or a stress reaction, so the management of the injury must be the same as that of a stress fracture. The athlete was taken out of his sport, with his return determined by the speed of his recovery. Custom orthotics were ordered to address the bilateral pronation and the increased Q angles, which arc the underlying cause of this condition. The injury is treated with cold laser therapy, kincsiotaping. ice therapy at home and no activities until further notice. I tell patients the more frequently they come in over the next three to four weeks, the quicker the condition will heal, regardless of what the actual diagnosis is. Three to five treatments per week arc recommended. If the condition docs not improve significantly in 10-14 days, an MRI is ordered. The results on the MRI will not change the treatment protocols at all. it will only support the delay in healing and make the return to activity time 4-6 weeks instead of 1-3 weeks. Conclusion Lower leg injuries are epidemic in youth sports. To the best of my know ledge, there is no profession who considers biomechanics when diagnosing or treating these athletes, yet it is fault) biomechanics that is the underlying cause to many of these injuries. A digital foot scan with lower extremity bio-mechanical testing, including Q angles, leg length, and joint mobility tests, should be considered on every middle and high school athlete prior to seasons beginning, with appropriate recommendations given, especially the recommendation of custom orthotics. A chiropractor should never refer this patient out. Dr. Maggscurrentlypracticesfiill lime, while also lecturing forFoot Ix^velers. He is the developer ofThe Structural Managements Program, asu ell as llie 10 Week ll'ehinar Series, "How to Build Your High School'Athlete Practice ". He coil be reached al l-51H-393-6566orRwmingDr(q)pol.coni Hiswebsiteis w\\w:Stnictural\ ianagement.com.