In chiropractic school, I was taught that we don’t treat symptoms; we treat the cause. After working with over 240 clinics in 45 states with Disc Centers of America, I have found that many doctors primarily focused on symptoms before working with us.
You may ask why I say that. Well, if the patient has a bulge or herniation, can you diagnose it simply from an X-ray? Does it make more sense to order an MRI if the X-ray shows a degenerative pathology? In the medical orthopedic world, this is considered a common procedure. The key to everything that we do is to be the best doctors, not the best salesperson.
It is fair to say that all fields and industries — medicine, commerce, finance, or government — harbor many who are ethical and well intentioned, as well as some who are greedy and unscrupulous. It is not always easy to tell one from the other in advance or even in retrospect.
We are proud that DCOA doctors are pathology driven instead of being money driven. If a patient is suffering from back pain, that is a symptom, but what if the cause is a bulge or herniation? How would you treat the patient? What about Cox therapy? What about Thompson terminal point technique? It is your job to know the best form of treatment for any individual case and that no two cases are the same.
Back trouble, in all its permutations, costs the United States roughly hundreds of billions of dollars a year. Some research articles state that more is spent annually on back issues than on cancer treatments, coronary artery disease, and acquired immunodeficiency syndrome (AIDS) combined.
On a per capita basis, other nations also pay hefty bills, chiefly the United Kingdom, Australia, Canada, Germany, Sweden, Denmark, the Netherlands, China, and South Korea. When I did my first Internet search, I had no idea that I’d spend six years studying this topic. Nor did I realize that in the interim, procedures that had been upheld for decades as the gold standard in spine care would be relegated to the dusty and crowded shelves of misguided medicine.
Doctors, what is your go-to technique for a disc problem? Many spine surgeons prefer a lumbar spinal fusion or a microdiscectomy. Primary care doctors often order a med dose pack or prescription opioids, which is one of the causes of our opioid epidemic. Most interventional pain physicians who perform epidural spinal injections learn that their shots don’t work. Epidural injections are not even approved for back pain, so it’s done as an off-label procedure.
Federal prosecutors punish device manufacturers for selling spinal instrumentation that is inadequately tested. Painkiller manufacturers and the U.S. Food and Drug Administration are tucked into bed with each other, working the drug approval process without regard for patients’ best interests.
Where did this surgical revolution begin? Everything changed in 1934 at Massachusetts General Hospital in Boston. In an effort to resolve a male patient’s back and leg pain, a neurosurgeon and an orthopedist successfully removed what they believed was a spinal tumor. The pain relented, but when the physicians examined the tissue, they realized that instead of cutting out a tumor, they had excised one of the 23 intervertebral discs that act as cushions between the bones of the human spine. The surgeons — William Jason Mixter and Joseph Barr — knew they were onto something. They were barely able to contain their enthusiasm for the procedure they described as “discal rupture.”
That was done prior to MRIs being an accepted medical procedure, and often, surgeons went in without fully knowing the patient’s complete diagnosis. Norman Shealy, MD, PhD, trained partially at Harvard, and he said that during his first surgery, he knew it was not the answer. He made it his lifelong quest to find a more effective nonsurgical, noninvasive back pain treatment with significant results.
Dr. Shealy went on to publish about 500 papers and many books. He worked diligently on developing nonsurgical spinal decompression, and he assisted in writing the protocols that we teach at Life University’s national certification program. In our conversations, Dr. Shealy noted that he was not a fan of epidurals; he preferred ID therapy and nonsurgical spinal decompression. He is best known for the Shealy-Bergmeier study.
In a 2015 review of medical literature, I was first amazed to learn the Agency for Healthcare Research and Quality had found no evidence that epidural steroid injections were effective in treating symptoms of spinal stenosis or typical low back pain. Even in the presence of a recent disc herniation and ensuing sciatica, the benefits of injections were small and not sustained over time.
That news followed on the heels of an FDA statement warning that injection of the active medication in these shots — glucocorticoids, a class of corticosteroids — into the epidural space of the spine could result in rare but serious neurological problems, including loss of vision, stroke, paralysis, and death.
Based on those and other findings, the Journal of the American Medical Association (JAMA) advised physicians to refrain from recommending injection therapy to patients with any kind of chronic back pain. That did not go over well with the doctors known as “interventional pain physicians” who make a living performing such procedures. In the United States, more than 10 million epidural steroid injections are delivered each year, a number that makes them the bread and butter of interventional pain management.
Whether the approach is transforaminal or interlaminar, some research shows that a quarter of epidural steroid injections miss their targets. Why? In “blind” injections performed without fluoroscopic guidance, the needle is incorrectly placed in up to half of epidural steroid procedures.
In roughly 6% of epidural steroid injections (a number that sounds small but is not because thousands of injections are delivered daily), the needle nicks the dura mater, the sturdy sleeve surrounding the spinal cord, allowing cerebrospinal fluid to leak. There is a great Dr. Oz video we show at The Chiro Event. Doctors who want to learn more about the treatment of disc injuries should attend and can learn more at TheChiroEvent.com.
Some epidural injuries can be serious. Often, side effects result in a severe headache, which goes away after the patient lies flat for a couple of days. Sometimes, like with San Francisco Warriors Coach Steve Kerr, a patient has a cerebrospinal leak. Then, a second procedure, known as a “blood patch,” is used to stop the leak of cerebrospinal fluid.
However, when the needle actually punctures the dura mater, it’s a different story. Then, the payload of glucocorticoid and anesthetic may be delivered into a region of fragile nerve tissue called the subarachnoid space. From there, the cerebrospinal fluid, bearing its toxic load, circulates to the brain, where the cortisone solution efficiently strips the insulating (and essential) myelin layer off neurons.
One result is “adhesive arachnoiditis,” a condition so grossly debilitating that neurologist Dewey Nelson described it as akin to “having a blowtorch up your rectum. It binds the nerves, like gunky cooked spaghetti, and the result is unrelenting pain that may last for a lifetime.” When I first watched this with a patient at the national certification program, I knew that I would never be a proponent of epidurals.
Our goal as chiropractors is to find the cause of the patient’s back pain. Dr. Bard and I, along with my son, Dr. Jason Kaplan, espouse repeatedly that a subluxation becomes a bulge, which becomes a herniation. The key is not letting that herniation rupture and getting the patient on nonsurgical spinal decompression before the patient is found on the floor writhing in pain with a ruptured or sequestered disc.
The lumbar spine is a frequent site of low back pain. The lumbar spine is made up of five vertebrae separated by intervertebral discs and the sacrum, which consists of five bones fused together. Each lumbar vertebra has a structure sharing several common factors:
Body (bearing the weight)
Pedicles
Laminae
Transverse processes
Spinous process
Superior/inferior articular processes
The pedicles and laminae form the neural arch and vertebral foramen. When all the vertebrae are aligned, this foramen forms the spinal canal and creates a body corridor for the spinal cord and the spinal nerves of the cauda equina.
Intervertebral Disc
The primary joint of the spine is the intervertebral disc, which consists of the annulus fibrosus, or the 10-20 concentric rings on the outside. These are known as lamellae, and their fibers are arranged at right angles to each other. They are firmly attached to the adjacent vertebrae and hold two vertebrae together.
The lamellae can suffer gap defects, not completely enveloping the nucleus pulposus, and these defects contribute to painful annular tears and disc herniations. Tears can be helped by class 3 or higher laser.
The end plates of discs are not as well attached as the annular fibers, and some research has shown that even mild trauma can cause separation from the vertebrae. These end plates act mainly like semipermeable membranes, allowing the diffusion of nutrition and waste products.
The nature of the end plate does not allow the movement of larger molecules, like the proteoglycans that maintain the nucleus pulposus. Because the nucleus pulposus is avascular, it must get its nutrition via the segmental vertebral blood supply. Only the outer third of the annulus receives a blood supply, and the end plate receives it from the vertebral body.
The center of the disc is a jelly-like, almost liquid substance called the nucleus pulposus, which holds the two vertebrae apart and permits movement between the two bones. The discs of the lumbar spine are taller than the cervical and thoracic ones and more vulnerable to injury. They contain 65% proteoglycans, which have a great affinity for water (their water content can be about 80%).
The zygapophyseal (facet) joints are behind the disc. The superior and inferior articular processes are bony projections that form these facet joints above and below. These are synovial joints, and the alignment of the facets defines the types of movement that will be permitted at that level of the spine. In the lumbar spine, they are in the vertical plane on an anteroposterior alignment, allowing flexion/extension and side-bending but very little rotation. The discs are cartilaginous, mainly avascular, and, like other cartilaginous tissues, slow healing if damaged. This is why checking range of motion during your examination is so important.
Zygapophyseal (Facet) Joints
In addition, the spine’s bones are shaped so that there are holes where they are typically aligned for the mixed spinal nerves to emerge from the spinal canal — the intervertebral foramina. This foramen enclosed the exiting nerve root and the delicate dorsal root ganglion (DRG). The DRG contains all the sensory nerve cell bodies. Anatomical variations show that the DRG can be inside or outside the intervertebral foramen. Any restriction of the intervertebral foramen’s space (through wear and tear, changes, or disc lesion) can upset the course of these delicate nerves.
Nerves of the Lumbar Spine
The vertebral canal encloses the thecal sac (dura mater), which, in turn, houses the spinal cord and spinal nerves. It extends from the base of the brain stem (the foramen magnum) down to the level of L1. There are “expansions” in the cervical and lumbar regions, reflecting the more significant activity and demand.
The dura mater is located within the spinal canal, a waterproof sac enveloping the spinal cord and spinal nerves. The arachnoid mater is on the inside of the dura and held against it by the presence of CSF in the subarachnoid space. The pia mater is outside the spinal cord and follows its convolutions. Even though the dura is a robust structure enveloping all this, specializations of the pia mater penetrate the dura, appearing as 21 pairs of denticulate ligaments that help anchor the spinal cord in the spinal canal.
The spinal cord ends at the level of L1. The remainder of the spinal canal is occupied by the spinal nerves continuing caudad to their level of exit from the spinal canal. The dura ends at S2 with its other fixation points at the foramen magnum and C2. The pia pierces the dura and continues to its final attachment at the coccyx, while the cord ends at the conus medullaris at the level of L1. Below that, the spinal nerves continue down to their level of exit as the cauda equina.
The nerves that leave and enter the lumbar spine control the trunk, lower extremities, and autonomic function. Suppose an injury occurs to any of these nerves. In that case, there can be a consequent effect — pain, loss of motor (muscle) function, loss of sensory sensation like light touch, pressure, temperature, vibration, and autonomic function (control of blood vessels size and sweating), or even cauda equina syndrome (loss of bladder and bowel control).
Someone may also experience complex regional pain syndrome (CRPS), a chronic pain condition most often affecting one of the limbs (arms, legs, hands, or feet), usually after an injury or trauma to that limb. CRPS may cause the lower extremities to swell, be very hot, and be sensitive to touch and sweat, which is why neuropathy is often associated with disc injuries.
At Life University in February, we will be conducting a certification on the neuropathy-decompression connection. Please watch your email and The American Chiropractor magazine for updates on this groundbreaking seminar.
Nerves Supplying the Disc
Everyone who presents with back pain announces that they have a “disc out of place.” That is an overgeneralization, but what are the mechanics of low back pain if a genuine disc pathology is present?
A different nerve pathway innervates each region of the disc, a phenomenon that occurs in no other structure in the body. The sinuvertebral nerve innervates the posterior and posterolateral regions of the disc.
The lateral disc by the gray ramus communicans (a sympathetic nerve of the autonomic system). The anterior disc by the sympathetic branches of the sympathetic trunk or ganglion.
The meningeal branches of the spinal nerves (also known as recurrent meningeal nerves, sinuvertebral nerves, or recurrent nerves of Luschka) are several small nerves that branch from the spinal nerve near the origin of the anterior and posterior rami but before the rami communicans branch. They then reenter the intervertebral foramen and innervate the facet joints, the outer third of the annulus fibrosis of the intervertebral disc, and the ligaments and periosteum of the spinal canal, carrying pain sensation. The nucleus pulposus of the intervertebral disc has no pain innervation, being both avascular and aneural.
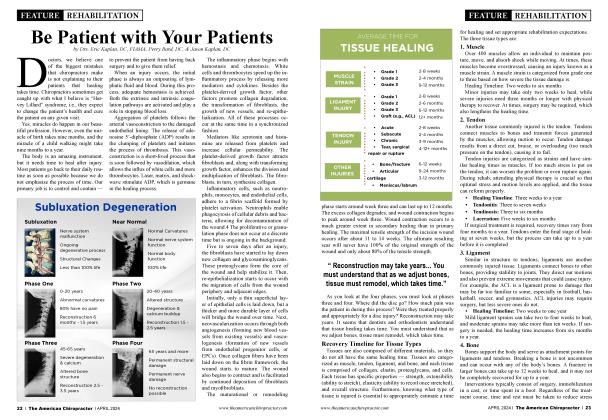
The true pain sensors of the disc (the free nerve endings of the nociceptors) are shown as yellow dots and have a greater concentration in the posterior and posterolateral aspects of the annulus of the disc as compared to the lateral and anterior regions. This suggests that the posterior and posterolateral regions of the disc are more sensitive to pain and possibly to the development of chronic back pain.
Annular tears and other types of disc lesions are found most frequently on the posterior and posterolateral regions of the disc. It would seem appropriate to focus on the sinuvertebral nerve, the primary nerve that carries pain sensation away from this area.
The sinuvertebral nerve has a bilateral origin and looks like a wishbone because it arises from both the ventral ramus (a somatic nerve) and the gray ramus communicans of the sympathetic ganglion (an autonomic nerve). This nerve innervates the posterior outer third of the disc at the same level and the same areas of the level above (e.g., the L4 sinuvertebral nerve innervates the posterior annulus of both L3 and L4).
Other opinions claim that one nerve can innervate three levels. This suggests that there can be “confusion” in the subjective experience of a painful disc since L3 and L4 are wired together (so if a person points at the pain in their back, the lesion may not be at that level). Hence, if a disc lesion is present, the sensation can enter the cord at one or more levels (myelomere). From there, the nerves decussate, travel up to the thalamus, and then onto the sensory cortex.
Despite extensive research, the precise pathway of the pain signals from the sinuvertebral nerves is uncertain. (This is frustrating to the orthodox medical world and its endeavors in injectable pain reduction). Logic would have us believe that pain signals would take the shortest pathway to the dorsal root ganglion (DRG), but apparently, it takes a more convoluted route. Using L4 as an example:
The sinuvertebral nerve goes to the gray ramus communicans (GRC).
The GRC to the sympathetic ganglion of L4.
The sympathetic ganglion of L4 up to the sympathetic ganglion of L1 or L2.
Across the white ramus communicans (WRC), which are only present at L1 and L2.
The WRC to the same level ventral root of the spinal nerve of L1 or L2 to the DRG of L1 or L2.
The DRG of L1 or L2 to the spinal cord at the L1 or L2 myelomere.
The spinal cord to the sensory cortex.
This hypothesis seems to be confirmed by the Nakamura study (1996) with L4 and L5 discogenic low back pain. Thirty-three patients with diagnosed L4 and L5 annular tears or herniation (all confirmed on MRI) were treated with selective nerve root block, using lidocaine injected at the L2 intervertebral foramen (i.e., close to the DRG). The theory was that blocking the L2 DRG would block pain sensation from L4 and L5 disc lesions, and the patient would experience less pain and increased function.
The theory was proven to be accurate when, within 15 minutes of the selective nerve root block, all the patients had experienced a reduction in subjective low back pain. They also had an increased ability to remain flexed at the waist in the standing position (static flexion test, which is challenging to perform in patients with disc lesions). Seventy-nine percent of this group experienced a complete or near-complete reduction of low back pain.
The authors suggested that discogenic low back pain is transmitted nonsegmentally by visceral sympathetic afferents, mainly through the L2 spinal nerve root (to the right). This may be perceived as referred pain in the L2 dermatome. Discogenic low back pain may be a type of visceral pain. Injection of the L2 spinal nerve root is a possible diagnostic tool and could be used for the conservative treatment of discogenic low back pain. As pain is being transmitted via visceral afferents, it can be interpreted (felt) as a type of visceral pain. Visceral pain, such as tummy ache, can be quite vague and tends to move around a bit in its location. Does that sound familiar?
Such pain can cause guarding of the muscles in those areas of referral, causing a persistent tension pattern therein, even establishing reflex patterns to maintain these patterns effectively. Persistent tension patterns can become chronic and predispose to degenerative changes in the areas affected, such as low back, hips, etc. The next questions to ask are: What causes the pressure in the disc, and how can it be reduced?
How Do We Know This for Certain?
So, how do we know that pain signals are not transmitted via the simple route described — same level disc, sinuvertebral nerve, same level ventral ramus, same level DRG?
Some disc surgeries have been performed under local anesthetic (i.e., the patient was awake). One subject was experiencing sciatica along with low back pain. During the discectomy procedure, it was demonstrated that by anesthetizing the inflamed nerve root at the same level of the disc herniation (i.e., the one causing sciatica), the patient felt relief in the radiating leg pain but no relief of the low back pain. They concluded that the low back pain signals were not traveling through the same level of the anesthetized nerve root; if they were, the low back pain would also have been relieved.
Pathophysiology
Doctors have tried treating disc problems for centuries. Prior to Dr. Alan Dyer’s (DC, PhD) original approach toward nonsurgical spinal decompression, there was no standard treatment. In the early part of the 19th century, intervertebral disc protrusion and subsequent pressure on the sciatic nerve roots were thought to be the likely source of sciatica and were hard to diagnose. The diagnostic test of choice used to be a myelogram, which usually was negative. When I graduated from chiropractic school in 1978, MRIs were not yet available.
Prior to decompression, the patient was often referred to the hospital where traction was administered. I once visited a family member, and the apparatus was quite archaic. They would simply hang weights from the patient’s legs, and the nurse or doctor would continually add more weight. Then, Drs. Alan Dyer and Norman Shealy came along.
Early studies showed disc traction was ineffective, and surgery became the popular way of treatment in the medical world. The medical community believed surgical removal of the disc would relieve the pressure on the nerve. By the mid-19th century, many publications presented arguments that pressure on nerves leads to loss of function and rarely to pain. Multiple studies have shown that patients are frequently asymptomatic despite having significant disc pathology.
Pain is only one indicator of DDD, and often, pain only surfaces at a late stage in the pathology. Early detection creates better results with any form of treatment. Remember, patients who have symptomatic disc herniation may not experience relief from the removal of disc material or other causes of compression, while others experience significant relief in the absence of any intervention. Although the pathophysiology is still not clearly understood, evidence suggests that the nucleus pulposus triggers an inflammatory response in sciatic nerve roots and may lead to pain.
Contrary to previous theories, multiple factors, including inflammation, abnormal immune factors, and mechanical compression of the nerve, are likely involved in producing pain. Multiple studies have shown that patients are frequently asymptomatic despite having significant disc pathology.
In one major study, Dr. Shealy showed that 86% of ruptured intervertebral disc (RID) patients achieved “good” (50-89% improvement) to “excellent” (90-100% improvement) results with decompression. Sciatica and back pain were relieved. “Of the facet arthrosis patients, 75% obtained ‘good’ to ‘excellent’ results with decompression.” C. Norman Shealy, MD, PhD, and Vera Borgmeyer, RN, MA. Decompression, Reduction, and Stabilization of the Lumbar Spine: A Cost-Effective Treatment for Lumbosacral Pain. American Journal of Pain Management Vol. 7 No. 2 April 1997.
Spinal decompression therapy is now making its move in the back world. We have consistently observed how conservative treatment for intervertebral disc herniation and IDD therapy, along with decompression, is setting a new standard. Spinal decompression therapy reduces pressure on the intervertebral disc by supplying nutrients and oxygen to the intervertebral disc.
It creates a state of nongravitation or negative pressure by adjusting the direction and angle of traction to suit the location of the intervertebral disc, which is the target of the treatment. That, in turn, reduces the pressure inside the intervertebral disc by gradually and softly increasing a specific part of the intervertebral disc through the decompression of a precise part of the lesion. This was first done by video fluoroscopy, which is included in the Ramos and Martin study.
The Boxell and Martin study stated, “The disc has the ability to repair itself.” Is that not simply the beauty, the paradigm, the essence of chiropractic? The power that creates the body has the power to heal the body.
Sometimes, we need to utilize a thrust or an adjustment. Sometimes, we need to utilize proven modalities, like nonsurgical spinal decompression. Many of our clinics often add laser, shockwave, electroanalgesia, cryotherapy, etc.
Doctors, there has never been a better time for chiropractic than there is today. If you want to learn more, come to The Chiro Event. For more information, visit TheChiroEvent.com.
Dr. Eric Kaplan and Dr. Perry Bard, are business partners of over 32 years. They have developed Disc Centers of America & Concierge Coaches. Currently, they have over 150 clinics using their Disc Centers of America brand and lead ongoing success training events throughout the year. For more information on coaching, spinal decompression, or seminars, visit www.thechiroevent.com or www.decompressioncertified.org, or call the Chiropractic Q&A Hotline at 888-990-9660.
Dr. Jason Kaplan is a graduate of Parker University. Along with his wife Dr. Stephanie Kaplan, they practice in Wellington Florida. Jason is an Instructor for Disc Centers of America, one of the Nation’s largest collection of doctors specializing in Disc Injuries. He has been recognized and honored by the International Disc Education Association and teaches technique at the National Certification Program at Life University and is considered a Master on Non Surgical Spinal Decompression, www.wellingtondisccenter.com.