ICD-10 Coding for Scoliosis
DOCUMENTATION
Dennis Woggon
Scoliosis is a neuromusculoskeletal disorder that may be caused by environmental and genetic factors, involving vestibular and neurological changes, hormonal and ligamentous influences, and alterations to normal spinal biomechanics. Every year, almost thr ee million scoliosis patients visit chiropractors1. Scoliosis is the most common spinal deformity, and perhaps the most complex. ICD-10 coding11 for scoliosis can also be complex. This article presents important points to remember when using the new ICD-10 codes for scoliosis.
First, the scoliosis must be defined by when it was initially diagnosed, and not when the patient presents to your office. For example, a 65-year-old patient who was diagnosed with
idiopathic scoliosis as a teenager would be listed using the following code: adolescent idiopathic scoliosis (M41.129).
Second, the appropriate cause for the scoliosis must be determined. Adolescent idiopathic scoliosis (AIS) is the most common, but if the scoliosis is secondary to a pathological or disease process (congenital malformation, cerebral palsy, etc.), that must be coded first. Congenital scoliosis due to congenital bony malformation (Q76.3) would be the appropriate code to use for an individual of any age whose scoliosis developed due to a hemivertebra or other bony malformation that was present at birth. Unlike idiopathic cases, congenital scoliosis cases never spontaneously resolve.
Third, the location of the scoliosis must be taken into account. Scoliosis is defined by the end vertebrae used to measure the Cobb angle; a case of scoliosis measured from T5 to T12 would be considered thoracic region, whereas a curve measured from T7 to F3 would be thoracolumbar.
It should be noted that the clinical notes must reflect the diagnosis. Any instances of the terms “cervicodorsal” or “lumbodorsal” in your notes should be replaced with “cervicothoracic” and “thoracolumbar” in order to be consistent with the diagnosis. The term “dorsal” should only be utilized when referring to a location toward or on the back of the body (contrasting with “ventral”).
Infantile idiopathic scoliosis (M41.00) is defined as a case of scoliosis unaccompanied by congenital abnormalities that is detected from birth up to three years of age. It is more common in males than in females. Many cases of idiopathic infantile scoliosis tend to spontaneously resolve within a few years, but those that do not stand a great risk of progressing to severe levels later in life.
Infantile idiopathic scoliosis
• C ervical region - M41.02
• C ervicothoracic region - M41.03
• Thoracic region - M41.04
• Thoracolumbar region - M41.05
• Fumbar region - M41.06
• Fumbosacral region - M41.07
Juvenile idiopathic scoliosis (M41.ll) is diagnosed from three to nine years of age. The prognosis is poorer in younger patients because scoliosis progresses at a higher rate when the patient has growth potential remaining.
Juvenile idiopathic scoliosis
• C ervical region - M41.112
• C ervicothoracic region - M41.113
• Thoracic region - M41.114
• Thoracolumbar region - M41.115
• Fumbar region - M41.116
• Fumbosacral region - M41.1174
Adolescent idiopathic scoliosis (M41.12), commonly abbreviated as AIS, is diagnosed from 10 to 18 years of age. It is often quoted that AIS comprises 80% of all scoliosis cases. One should keep in mind that school scoliosis screenings are typically conducted on adolescents, and that we generally stop looking after then.
Adolescent idiopathic scoliosis
• Cervical region - M41.122
• Cervicothoracic region - M41.123
• Thoracic regionM41.124
• Thoracolumbar region - M41.125
• Lumbar region - M41.126
• Lumbosacral region - M41.127
The incidence of scoliosis in adolescents is reported to be between 2 to 4.5%. When adults are examined for signs of scoliosis, the incidence has been reported at 12%lh, 32%1V, 48%v, or even 68%V1 over 60 years of age. B.J. Palmer said one out of three people has scoliosis". Screening may miss many mild cases of scoliosis, or scoliosis could be developing after the screenings. In either case, it illustrates the importance of screening for scoliosis in all of your patients and not just adolescents. When conducting scoliosis screenings, be sure to use a scoliometer because the device significantly improves the effectiveness of the exa.miua.tiou.
Other idiopathic scoliosis (M41.2)
is the correct code to use for any case of scoliosis that was not detected before the patient reached skeletal maturity (typically age 18) or if the onset is unknown. This includes cases of degenerative (or de novo) scoliosis, which tend to arise in the lumbar spine in individuals past the age of 40 as a consequence of intervertebral disc degeneration and a loss of integrity of the annulus fibrosus.
Degenerative scoliosis is often accompanied by lateral listhesis (sideways slippage) of the apical vertebra, as well as thin discs, osteophytes, and other signs of spinal degeneration. It is important to recognize degenerative scoliosis as a distinct and separate disease entity from adult idiopathic scoliosis. Although both could be considered chronic conditions, the circumstances under which they arose and their subsequent effects upon the body
and spinal column will be very different, and thus require different rehabilitative strategies.
Degenerative disc disease
• Cervical DDD - M50.31 - C2/3 or C3/4
• Cervical DDD - M50.32 - C4/5, C5/6, C6/7
• Cervical DDD - M50.33 - C7/T1
• Thoracic DDD - M51.34
• Lumbar DDD - M51.36
For adults with idiopathic scoliosis, it is common to find disc degeneration more frequently than the average population. As mentioned previously, however, be sure to differentiate between disc degeneration caused by idiopathic scoliosis and scoliosis caused by disc degeneration. In either case, though, if disc degeneration is present, the codes for disc degeneration (M50.3, M51.3) would also be utilized.
Neuromuscular scoliosis (M41.4) is
the correct code to use for cases of scoliosis associated with neuromuscular disorders, such as cerebral palsy, Friedreich’s ataxia, or poliomyelitis. If the patient has had surgery for their scoliosis, the correct code is Z98.1 - Arthrodesis status.
Subluxations obviously exist throughout the scoliotic spine, including the upper cervical region. Chiropractic science has long recognized the influence of the upper cervical spine upon the cerebellum and the postural muscles of the body.
Subluxation syndrome
• Cervical subluxation - M99.11
• Thoracic subluxation - M99.12
• Lumbar subluxation - M99.13
• Sacral subluxation - M99.14
• Pelvic subluxation - M99.15
Segmental and somatic dysfunction
• Segmental and somatic dysfunction, cervical - M99.01
• Segmental and somatic dysfunction, thoracic - M99.02
• Segmental and somatic dysfunction, lumbar - M99.03
• Segmental and somatic dysfunction, sacral - M99.04
• Segmental and somatic dysfunction, pelvic - M99.05
The diagnosis of subluxation syndrome (M99.0) or segmental and somatic dysfunction (M99.1) (or both) should be the primary diagnosis for all scoliosis patients. If indicated, this can be correlated with sprain/strain of the ligaments.
The ICD-10 codes for sprains are cervical, (S 13.4); thoracic, (S23.3); ribs, (S23.41); lumbar, (S33.5); and sacroiliac, (S33.6). There are usually rib subluxations and sprains associated with the rib arch.
Sprains/strains
• Sprain of ligaments of cervical spine - S 13.4
• Sprain of ligaments of thoracic spine - S23.3
• Sprain of ribs - S23.41
• Sprain of ligaments of lumbar spine - S3 3.5
• Sprain of sacroiliac joint - S33.6
Note that sprain/strain is not the same as ligament laxity (M24.28). Ligament laxity is considered more severe due to the inherent instability.
Ligament laxity and joint hypennobility is commonly found in scoliosis. The combined clinical observations and experiences of scoliosis chiropractors using digital motion X-ray (DMX) technology have revealed that this ligament laxity extends to the upper cervical spine. This can also be caused by birth trauma, car crashes, or other injuries. Manual manipulation is contraindicated in areas of hypennobility. Only lateral cervical flexion/extension X-rays, A-P open-mouth lateral flexion X-rays, and digital motion X-ray technology can detemnine if instability or hypennobility, or both, exist in the cervical spine. Positive findings would indicate a diagnosis of ligament laxity (M24.28). This could relate to the alar ligament, transverse ligament, anterior/posterior longitudinal ligaments, and capsular ligaments.
Paraspinal muscles on the concave side of scoliosis exhibit hyperexcitability when the Cobb angle exceeds 30 degrees™'. In a “typical” scoliosis with a right thoracic Cobb angle and a left lumbar Cobb angle, there would be muscle tightness (not spasm) in the right trapezius and left quadratus lumborum. This would be coded as contracture of muscle, multiple sites (M62.49). Muscle spasm is acute, whereas muscle guarding is a chronic condition that develops as the fast-twitch (type II) fibers transform into slow-twitch (type I).
The normal sagittal curves of the spine give the spine strength and flexibility. When the healthy sagittal curves are lost, the spine becomes more susceptible to injury and the development of spinal deformity. Almost all scoliosis patients will have a loss of the thoracic kyphosis'x, and many also have a cervical kyphosisx. If kyphosis is present in the cervical spine, the ICD10 code (kyphosis - cervical region, M40.292) should be used.
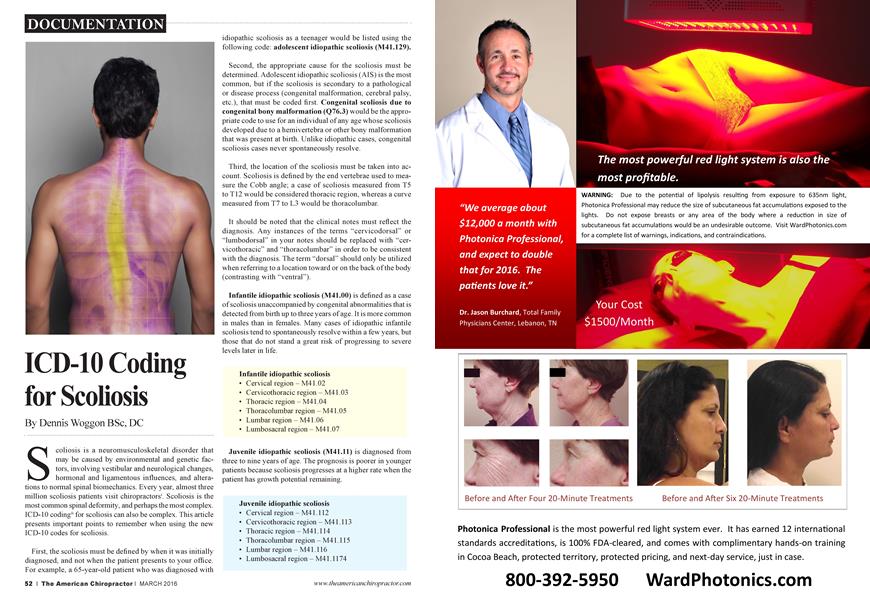
While we tend to focus on the primary structural curve when evaluating a scoliosis, it is important to take the compensatory curvatures into account as well. The primary righting reflex of the body is the eyes, and the head and neck will always adapt
to keep the eyes level to the horizon. In the case shown, the tendency is to diagnose it as a single thoracic scoliosis (Ccurve), from T6 to T12. However, there aie also cervicothoracic and lumbar curvatures from C7 to T6 and LÍ to L4. In the case of an adolescent with idiopathic scoliosis, this would be correctly coded as AIS - cervicothoracic region (M41.23), AIS - thoracic region (M41.24), and AIS - thoracolumbar region (M41.25).
The understanding of scoliosis and the ICD-10 codes is important to the chiropractic profession if we want to be “the spinal experts.” Scoliosis is diagnosed when there is a Cobb angle larger than 10 degrees. Documentation of the scoliosis patients verified by the ICD-10 codes will verify our treatment of scoliosis patients. The ICD-10 codes were implemented by the World Health Organization (WHO) to monitor the health status of 117 countriesiA Utilization of these codes will have an international effect.
Chiropractic care of mild scoliosis could be considered a success if the Cobb angle does not increase while under treatment. This is the goal of bracing. If we can reduce and stabilize the scoliosis, that will be even better. The true goal of chiropractic scoliosis treatment should be to reduce the Cobb angle and to provide the patient with the optimal quality of life. This is possible with advanced chiropractic treatment developed specifically to help people with scoliosis.
The CLEAR Scoliosis Institute specializes in comanaging chiropractic scoliosis patients with other doctors. You can find a CLEAR doctor to help you with your scoliosis patients at www.clear-institute.org. For more information, go to www. clear-institute. org.
References:
i. Christensen MG, Kerkhoff D, Kollasch MW. Job analysis of chiropractic 2000. National Board of Chiropractic Examiners, Greeley; 2000.
ii. ChiroCode ICD-10 Coding For Chiropractic - 2nd Edition
iii. "Scoliosis screening of 3,000 college-aged women. The Utah Study - Phase 2”, Brigham Young University, Provo, UT, Francis RS. Phys Ther 1988 Oct;68(10):
iv. Adult scoliosis: Prevalence, SF-36, and nutritional parameters in an elderly volunteer population, 2005 May 1 ;30(9): 1082-5.
v. J Am Osteopath Assoc. 2013 Mar;113(3):210-4. Scoliosis Rates in Symptomatic Patients as Demonstrated With Weight-Bearing or Supine MR Imaging. Vogt MS, Gilbert JW, Windsor R, Mick GE, Richardson GB, Storey BB, Herder SL.
vi. 2005 May 1 ;30(9): 1082-5. Adult scoliosis: Prevalence, SF-36, and nutritional parameters in an elderly volunteer population.
vii. Chiropractic Technique, 1920
viii. "Motor Unit Analysis Of Paraspinalis Muscles In Idiopathic Scoliosis”, Koo, Cheng, Xia, Dept. Of Pediatrics, Prince of Wales Hospital, Chinese University of Hong Kong, Children's Hospital of Michigan, Wayne State University
ix. The pathogenesis of idiopathic scoliosis. Biplanar spinal asymmetry.
J Bone Joint Surg Br. 1984 Jan;66(l):8-15. Dickson RA, Lawton JÖ, Archer IA, Butt WP 1984
x. Momingstar MW, Stitzel CJ. The relationship between cervical kyphosis and idiopathic scoliosis. J Vertebral Subluxation Res. October 13, 2008; 1-4. -See more at: http://nwprc.coin/2012/07/neck-curve-linkedand-scoliosis/#sthash.xSIWsCdL.dpuf
xi. http://www.who.int/classifications/icd/en/
Dr. Dennis Woggon is the founder o f the CLEAR Scoliosis Institute and the St. Cloud Chiropractic Clinic. He graduated from Palmer College of Chiropractic in 1974. He is an international instructor for CLEAR Scoliosis Institute. He can be contacted at [email protected].