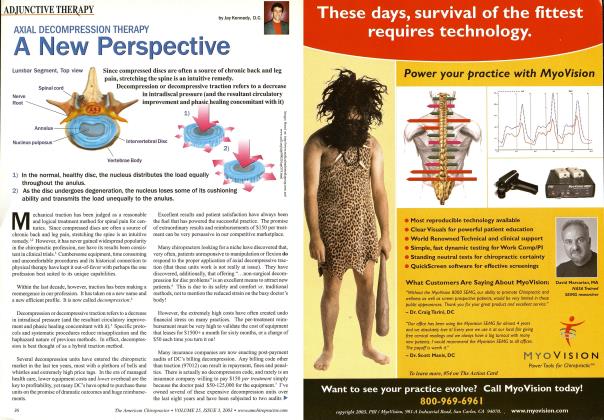
An cvidenced-based practice is defined as the conscientious and judicious use of current best-evidence in making decisions about patient care.1 Decisions about the delivery and provision of health-related services arc being increasingly driven by research, cost-effectiveness and the strength and weight of the available scientific evidence. The Cochranc collaboration library is a worldwide data base creating systematic reviews available to those interested in the available evidence (via systematic reviews) on innumerable health topics including traction (decompression). Axial traction/decompression is a passive modality and (like Ultrasound. LLLT& EMS) tends to have limited A-level (1++) research proving definitive efficacy without bias. As defined by various research networks that grade evidence, high-quality mcta-anah sis. systematic reviews of RCTs arc considered 1++ and have a very low risk of bias. They arc at the top of the research hierarchy. Systematic reviews of cohort or case studies, non-analytic studies and expert opinion come up at the lower end because bias is not controlled definitively.2 As has been stated by many insightful clinicians "lack of evidence doesn't prove evidence of lack." How ever it is disconcerting that such limited evidence exists for so much of what we do (considering much of what we do we've been doing for over seventy years). It may well be that we have simph not been looking at it in the right way. Heterogeneous and homogenous populations arc buzz words in back pain research and may continue to be the most common reason definitive answers of "who." "what" and "why" evade us. If a likc-population cannot be defined then the outcome can be inaccurate and biased. This docs seem to be the case with many studies on traction (and mam- on exercise and spinal manipulation as well). The CPR patient (clinical prediction rule) for manipulation is often different from the patient being offered manipulation at our clinics each day.' Best-evidence for manipulation is still in development though most of us tend to assume "manipulation is cvidcnccd-based" ... w hen in fact how and to whom it is delivered determines whether it is in alignment with bcst-cvidcncc. The most recent trials on traction also focus on classification (sub-grouping/CPR(s)) of patients ... again however the successful participants in these trials can be different from those we may be classifying for the therapy.4 The question in the title is commonly asked at seminars, that is. "do position-limited traction tables (typically supine only) align with the bcst-cvidcncc available for traction?" The answer, perhaps obviously, is no. The reason why such a question persists is because several manufacturers not only continue to perpetuate the notion that a supine-only traction table is decompression (harboring some "magic" machine attribute), but that it is also somehow technologically advanced. The short response to such marketing hyperbole and misdirection should be: From what evidence do you draw your conclusions? It clearh isn't the available pccr-rcvicwcd research or their own independent research. It isn't from the system that ostensibly ""created" decompression as a distinct clinical offering: the VAX-D. The VAX-D was prone-only and their seminal studies showing enhanced efficacy vs. "traction" units were all done prone.5 Nor is it from the vast majority of tables sold to DCs. MDs. PTs or hospitals over the last dozen years since the vast majority were both prone and supine. If we look, even in a cursory way at the available research, we sec a very strong case being made for prone trcatmcnt(s) and certainly a case being made tliat both prone and supine arc obviously necessary. No real, scientifically valid case can be made for limiting the therapy to just one position (Why would you limit manipulation or exercise to just one position?). Position and force arc really the only two variables a clinician controls. Suggesting there should be only one position (and that being determined by the manufacturers" whim) is as absurd as suggesting there should only be one specific force. Many years ago the term gravitational bias was used by Mathcws and others to describe the natural attribute of the nucleus in the prone position to "drift" or migrate toward the anterior (away from the distended posterior annulus). This is of course the P-A mobilization position used in innumerable PT treatments for disc hcrniation as well as the only position for flexion-distraction for nearly a hundred years. When we give a rudimentary thought to supine traction we see a less than ideal gravitational situation. In fact it is apparent that the main premise for any efficacy to anterior-migration of the posterior hernia is via the tautness or tensioning of the PLL... any centripetal effect is minimized by the crecp/migra- tion effect. And this particular phenomenon with the PLL lias vet to be specificalh demonstrated (and theoreticalh impossible with trans-ligamentous hcrniation). Problematically as well is that main supine-only systems suggest 20+ minute protocols. At that length of time certainly one anticipates more natural "gravity-biased" creep/migration of the nuclear material in the "wrong" direction. We have followed the lead of the research and expert opinions who continue to propose prone traction as the go-to position for most HNP conditions that demonstrate an extension directional bias/ preference. This is extremely common as well. Research confirms derangement syndromes (discal migration) that constitute some 87% of entrance complains for those seeking PT care for back and/or leg pain.'1 Of those at least 70% demonstrate a reducible hcrniation with an extension directional preference. Is it really sensible to consider (or be forced) to treat these patients supine ... Of course it isn"t. As a matter of fact, the research by Fritz ct al. 2007 utilized the prone position exclusively. When prone posture was untenable due to nerve-tension issues the tables caudle section was dcllcctcd to create tolerance via foraminal widening. Additionally, the majority of hcrniatcd discs occur in people under the age of 45.7 These "classic" hcrniations should, by the standard of best-evidence, be first disqualified from prone- position before defaulting to supine. I contend in classic HNP that younger age groups do not fare well with supine positional traction. There is a reasonable age-split in using prone vs. supine position based on these facts. Younger patients tend to need prone-positioning, older patients (and the elderly) more likely supine, though neither is exclusive. As we age. hcrniations per sc become far less common as degeneration, internal disc disruption, spondvlosis and desiccation increase. These conditions dont absolutely necessitate supine positioning but what they do demonstrate is that "decompression" as a phenomenon of traction may not be the operative benefit in the face of moderate or severe degeneration. That's why supine position in this older age group appears to be well tolerated and not apparently detrimental. Gay ct al. in the 2007 Spine discussed the fact that distraction predictably reduces nuclear disc pressure but this effect is dependent on the level of degeneration. In their study. 4 out of 8 moderately degenerative discs demonstrated "decompression": however, only 1 out of 7 severely degenerative discs had the same effect. Best evidence still may be weak or lacking regarding the long-term benefits of lumbar traction and who may be the ideal candidate: however, that traction should often times to be delivered prone to be the most beneficial and in alignment with the scientific evidence is unarguable. Dr. Kennedy has developed, tested and taught an effective, easy to learn decompression therapy technique. His pro- locols have been taught to over 4,500 chiropractors and physical therapists. In over 20 years of practice, he has owned and operated most of the decompression therapy equipment offered by a range of manufacturers. This has afforded him the position of having done JOO's of cross-comparison treatments with these units. He believes that it is imperative to "put the doctor into Decompression Therapy". References: 1. Sackett DL et al. Evidenced-based medicine: what it is and what it isn 't. BMJ 312; 71 1996. 2. Ibid 3. French SD et al. Reliability of chiropractic methods to delect manipulable lesions in cLBP. J.\lPT.\lay;23(4) 2000. 4. Clarke ./ et al. Traction for LBP; an updated systematic review (Cochrane collaboration). Spine Jim 15;31(14) 2006. 5. Gose E, Xaguszewski Wm (dept. of bioengineering U of Chicago). Xeurol Res; 20: 1S6-190. 1998 6. Heffort! C. McKenzie classification of mechanical spinal pain. Man Ther. 2008 7. Bogduk X. Adams M et al. The biome-chanics of back pain. Churchill Livingstone. 2007.