New worlds are forming in chiropractic. In the old world of chiropractic, PVA stood for “patient visit average.” In the new world and at the Disc Centers of America, it means “patient value average.”
What is a back problem worth to you? What is a neck problem worth to you? At DCOA, we are excited to be the first outpatient clinic specializing in disc injuries at Life University, the largest chiropractic school in the world.
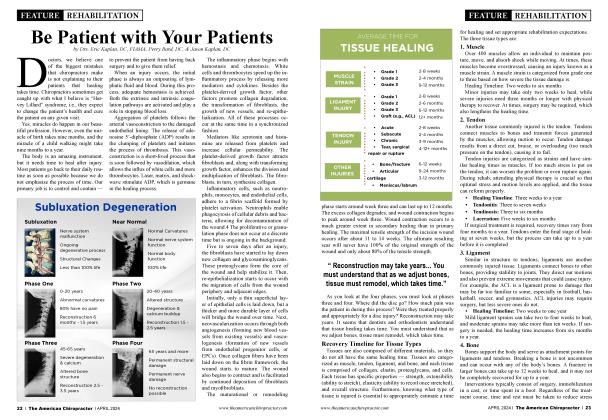
We specialize in and teach about the progression of the subluxation complex. A subluxation can become a bulge, and a bulge can become a herniation. There are now studies showing phenomenal success rates with spinal decompression, and Life University is committed to donating time, energy, effort, and money to research in this area.
We can discuss many studies — from the Dr. Yoakam study, Dr. Leslie study, Dr. McClure study, and, of course, Dr. Norman Shealy, MD, PhD, studies. We’ve written articles in the past about failed back surgery syndrome. Tiger Woods, who recently had a seventh back surgery, was just involved in another automobile accident. How will the hardware that was put into his back be affected?
• In the Journal of Neurological Research (volume 20, number 4, April 1998), researchers stated, “We consider decompression therapy to be a primary treatment modality for low back pain associated with lumbar disc herniation at single or multiple levels, degenerative disc disease, facet arthropathy, and decreased spine mobility. Physiology (pain and mobility) and pathology correlate imprecisely. We believe that post-surgical patients with persistent pain or ‘failed back surgery syndrome’ should not be considered candidates for further surgery until a reasonable trial of decompression has been tried.”
• In the Journal of Neurological Research (volume 23, number 7, October 2001), researchers stated, “For any given patient with low back and referred leg pain, we cannot predict with certainty which cause has assumed primacy. Therefore, surgery, by being directed at root decompression at the site of the herniation alone, may not be effective if secondary causes of pain have become predominant. Decompression therapy, however, addresses both primary and secondary causes of low back and referred leg pain. We thus submit that decompression therapy should be considered before the patient undergoes a surgical procedure that permanently alters the anatomy and function of the affected lumbar spine segment.”
• In that same volume of the Journal of Neurological Research, the senior lecturer of orthopedics at Sydney University stated, “Successful reduction of intradiscal pressures with decompression therapy represents a technological advance in lumbar spinal treatment and is likely to affect both the biomechanical and biochemical causes of discogenic pain.
Clinical studies have shown decompression therapy to be extremely effective in treating back pain. In a recent study published in Orthopedic Technology Review, decompression therapy was shown to be 86% effective in treating herniated and degenerative discs. Another study published in Anesthesiology News showed that after four years, over 91 % remained pain-free.
Decompression therapy should be considered first, before the patient undergoes a surgical procedure, which permanently alters the anatomy and function of the affected lumbar spine segment.”
TDC therapy is exclusive to Disc Centers of America and utilizes a traction decompression correlative (TDC) to create a form of decompression therapy. DCOA doctors are specifically trained and often certified versus others who use generic traction devices that cannot isolate a specific segment, which does not take the patient’s normal lordotic curvature into account.
DCOA’s patented TDC therapy allows discs to heal because the treatment stimulates the cartilage to regenerate — an act it cannot do on its own without the technology of TDC therapy. Spinal decompression utilizing TDC therapy is a result of specific traction that allows the nutrient-rich blood to fill the disc space, which fosters the healing response.
At Disc Centers of America, we understand that decompression is an event as a result of specific traction, which makes our technology so unique. TDC therapy can work on the segment that is involved and not alter healthy vertebrae.
TDC therapy is a proven, comprehensive treatment for the relief of neck and lower back pain. The purpose is to create spinal decompression by utilizing traction specific to the segment of involvement. TDC therapy offers a significant success rate; patients have experienced dramatic pain relief and healing.
This nonsurgical solution for disc disease, herniations, and associated pain is changing the way doctors now treat herniations. Endorsed by leaders of both the chiropractic and medical professions, TDC therapy is a proven system of protocols designed exclusively for Disc Centers of America. DCOA is already the only group of doctors that utilizes nonsurgical spinal decompression (NSSD), endorsed by Dr. Norman Shealy. How does TDC Therapy work?
TDC therapy utilizes computer technology that can customize and isolate segments of the lumbar spine and distract the vertebrae surrounding an injured disc by as much as 5 to 7 min over time. The 23to 30-minute treatment provides static, intermittent, cycling forces on structures that may be causing neck or lower back pain.
Disc Centers of America clinics utilize specific negative pressure that gently promotes the diffusion of water, oxygen, and nutrients into the vertebral disc area, thereby rehydrating the degenerated disc. The repeated negative pressure differential can promote retraction of a herniated nucleus pulposus (the elastic core of the intervertebral disc), facilitating an event we call decompression.
Utilizing specific biotechnology, TDC therapy works to reduce pressure on the vertebral joints, which will work to promote a retraction of herniated discs. This allows the body to promote self-healing and rehabilitation of damaged discs. As this event takes place, your body’s natural healing process will begin, and you will find a great reduction in pain.
Several sessions are required, customized, and specific to Disc Centers of America. TDC therapy works to achieve optimal results in a minimal amount of time. Rates and levels of improvement vary from patient to patient, often depending on the grade and level of your disc problem.
DCOA technology allows you to customize your treatment for each patient, store the data, and specifically treat the involved segment. Spinal decompression has been shown to:
• Enlarge the disc space.
• Reduce herniations.
• Strengthen outer ligaments to help move herniated material back into place.
• Reverse the high intra-disc pressures through the application of negative pressure.
Often, when there is a bulge or herniation, you can have an annual tear. Annular tears respond very well to laser therapy.
An annular tear is a rupture in the annulus fibrosis (AT). The annulus is the tough outer layer of your disc that contains the inner nucleus pulposis.
A tear in the AF can cause severe pain and even a radiating pain into your arms or legs. It can allow the inside jelly-like substance to push out and put pressure on the delicate spinal nerves, causing severe pain, although a tear may not cause any pain at all.
Truly, one of the most effective means of treating an annular tear is NSSD along with class IV laser therapy. Decompression can recreate the normal pumping action of the disc that creates osmosis and imbibition. It also allows us to rehydrate the disc and bring nutrients into the disc to help it heal the tear and restore normal function to the disc, reducing and eliminating the pain caused by a torn or degenerated disc.
A disc is a ligament, and ligaments have poor to no blood supply, which is why a sprain will heal slower than a fracture. A broken bone has a rich blood supply to allow it to heal faster than ligaments. The beauty of nonsurgical spinal decompression is that it helps give the discs the nutrients needed to heal. Class IV lasers can also help increase the microcirculation around the disc, further facilitating its healing.
An annular fissure or tear is a deficiency of one or more layers of the annulus fibrosus. Most annular fissures are asymptomatic, but some may be painful. Chronic pain due to annular fissures can be due to granulation tissue, in-growth of nerve endings near the dorsal root ganglion, or disc herniation of the nucleus pulposus. This activity reviews the evaluation and management of this condition, highlighting the role of the interprofessional team in providing care to patients affected by annular disc tears and improving long-term outcomes.
The annulus fibrosus is the type I collagen surrounding the nucleus pulposus in approximately 15 to 20 layers. Together, the annulus fibrosis and nucleus pulposus form the intervertebral disc between adjacent vertebrae.
The annulus fibrosus runs obliquely between edges of adjacent vertebrae, connecting the inferior endplate of the superior vertebra with the superior endplate of the inferior vertebra. The directions of the layers of the annulus fibrosus alternate, which adds to the strength of the annulus fibrosus.
Near the central region, the annulus fibrosus blends with the nucleus pulposus. The posterolateral aspect of the annulus fibrosus has a greater content of vertically oriented fibers, leading to relative focal weakness at the posterolateral aspect. This anatomy of the annulus fibrosus explains why most annular fissures are at the posterior or posterolateral aspect of the annulus fibrosus.4
The posterolateral aspect of the annulus fibrosus has a greater content of vertically oriented collagen fibers. In other regions of the annulus fibrosus, layers alternate obliquely oriented layers. Thus, in the posterolateral region, the vertical alignment of the fibers is more likely to allow for focal deficits of the annulus fibrosus and tearing or separation between the vertically oriented fibers.
Most annular fissures or annular tears are asymptomatic and discovered incidentally on imaging. If an annular fissure or tear is symptomatic, it may cause one of two findings: localized pain secondary to the tear or radicular symptoms secondary to irritation of the passing nerve root. The pain may either be acute if the tear occurs suddenly or more chronic if there is a slower development of the annular fissure.
If the annular fissure is locally symptomatic, it may cause localized deep pain that worsens with movements, which can stress or irritate the focal annular tear. In such cases, there is no radicular nerve involvement, and the physical exam may be unrevealing.
Sometimes the annular tear can irritate the traversing nerve and cause radiculopathy. If the annular fissure or annular tear is significant enough, disc material can hemiate to irritate or compress traversing nerves or the spinal cord. In either case, when the traversing nerve is irritated, it can cause radicular symptoms, including pain, paresthesia, or weakness, depending on the extent of nerve irritation or compromise.
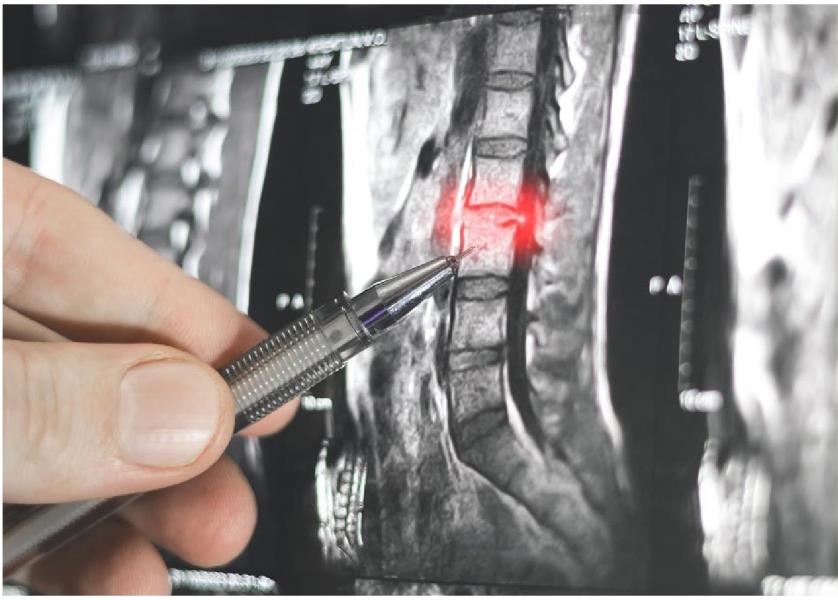
An annular fissure can be concentric, transverse, or radial in orientation and may involve some or all layers. On magnetic resonance imaging (MRI) T2 sequence, the annular fissure is hyperintense (bright) compared to the rest of the annulus fibrosus (which is normally hypointense or dark) due to the relative increase in water content at the fissure compared to the normal annulus fibrosus.7
If there is herniation of intravertebral disc material, there must be incompetence of the annulus fibrosus, and thus, an annular fissure or annular tear must be present, even if not specifically visualized on the imaging. Thus, an annular fissure or annular tear can be implicated any time intravertebral disc herniation is identified.
If a patient is unable to have an MRI, a computed tomogram (CT) myelogram may show nerve root or cord compression from a disc protrusion. The CT cannot identify the edema of an annulus fibrosus teaior fissure, and thus, it is less sensitive than MRI.
If there is disc protrusion or herniation, it is usually the protruding or herniated disc material that causes clinical symptoms. In such cases, the patient is treated for disc protrusion or herniation and not the annular fissure or tear.
Treatment options for disc protrusion or herniation include conservative measures of nonsteroidal anti-inflammatory medications, physical therapy, and local injections. If symptoms fail to improve, symptoms progress, or the patient develops weakness, surgical treatment options should be considered, including laminotomy, laminectomy, foraminotomy, discectomy, fusion, or some combination thereof. If a discectomy is performed, there has been no convincing evidence that closure of the annular fissure, tear, or annulotomy significantly affects the long-term outcome for the patient.
Annular tears are quite common and often associated with low back pain. The diagnosis of annular tears and their correlation to symptoms is not always easy. Many patients with mild annular tears have no symptoms, but some do present with excruciating low back pain with minimal evidence of an annular tear.
Thus, a thorough neurological exam is key. The decision to obtain imaging studies depends on the severity of symptoms. However, the treatment of annular tears also requires good clinical judgment. A number of patients do improve with conservative treatment like laser therapy.
Lumbar annular tears can be caused by several factors, including age-related degeneration, trauma, or repetitive stress on the spine. These tears often lead to the release of inflammatory chemicals that irritate surrounding nerves, resulting in pain and discomfort. In some cases, the tear can allow the inner disc material to protrude, leading to a herniated disc and further complications.
The symptoms of a lumbar annular tear can vary depending on the severity and location of the tear. Common symptoms include localized lower back pain, which may worsen with movement or prolonged sitting. Some patients may also experience radiating pain, tingling, or numbness in the legs, indicating nerve irritation or compression. Early diagnosis and treatment are essential to prevent the condition from worsening and improve the quality of life.
Diagnosing a lumbar annular tear typically involves a combination of physical examinations, medical history review, and imaging tests, such as MRI or CT scans. These diagnostic tools help in assessing the extent of the tear and its impact on surrounding structures. Once diagnosed, a tailored treatment plan can be developed to address the specific needs of the patient.
Laser therapy is simply a coherent light source that produces joules, or energy. Much of a laser’s biostimulatory effects and pain-relief aspects are absorbed in the skin and underlying tissues.
It is critical to use a high-powered laser, such as a class III or class IV laser (versus a class II), for its effects to penetrate deep into the tissues we are trying to heal. Class II lasers are good for dermatological conditions but will not be effective to treat tissues below your skin layer.
Class III and class IV lasers are an effective, noninvasive way to accelerate healing and repair body tissues. They alleviate pain, reduce inflammation, and speed up functional recovery.
The injured cells in your body respond to the deep penetration of laser photons, enhancing microcirculation and blood oxygenation to the compromised area, thus accelerating the rate of repair. Laser therapy is useful for alleviating neck, back, and knee pain, as well as repairing shoulder and rotator cuff injuries, providing relief for arthritis, and reducing inflammation and joint swelling.
For many patients, nonsurgical treatments can effectively manage the symptoms of lumbar annular tears. These conservative approaches aim to reduce inflammation, alleviate pain, and improve mobility. Physical therapy is often recommended as a first-line treatment, focusing on exercises that strengthen the core muscles, improve flexibility, and promote proper spinal alignment.
• Alleviates neck, back, and knee pain.
• Repairs shoulder and rotator cuff injuries.
• Provides relief for arthritis.
• Reduces inflammation and joint swelling.
According to a study in the American Journal of Pain Management, the nonsurgical spinal decompression (NSSD) provided good-to-excellent results for 86% of patients with herniated or ruptured discs and 75% of patients with facet arthrosis, as discussed in the Shealy-Bergmeyer study.
Let’s summarize:
• Spinal decompression was cleared by the Food and Drug Administration. Many doctors still advertise that it’s FDA-approved. Drugs are FDA-approved, but equipment is FDA-cleared.
• Many diagnoses are treated by NSSD and TDC therapy, including:
° Pinched nerve in the neck or low back
° Sciatica
° Herniated disc
° Bulging disc
° Ruptured disc
° Tom disc (or disc tear)
° Slipped disc
° Collapsed disc
° Disc protrusion
° Disc degeneration
° Degenerative disc disease
° Disc disease
° Black disc
Spinal decompression has been successful with even the most severe cases, even when nothing else has worked, including failed back surgery.
DCOA works closely with a team of medical doctors who follow protocols set up by the International Medical Advisory Board on Spinal Decompression. They also follow the protocols set forward by Dr. Norman Shealy, the board’s honorary chairman, a former Harvard professor, and probably the most published doctor in the world on spinal decompression.
DCOA doctors utilizing TDC therapy outline a detailed and specific approach prior to treatment, starting by determining the pain generator or cause via examination and diagnostic studies. A physician’s diagnosis focuses on determining the source of a patient’s pain. For this reason, the medical diagnosis of a patient’s neck pain, low back pain, leg pain, or other symptoms is based on more than just the findings from a diagnostic test, such as an X-ray, MRI, or CT scan.
Instead, DCOA healthcare professionals arrive at a diagnosis by synthesizing findings from a thorough review of the patient’s medical history, a complete physical exam, and, if appropriate, the results of one or more diagnostic tests. The objective of TDC therapy is to treat the cause of the problem, based on severity, through the Kaplan-Bard grading matrix or TDC grading system.
Prior to rendering TDC therapy, the following protocol is recommended:
• Medical history. The physician will take the patient’s medical history, such as a description of when the neck pain, arm pain, low back pain, sciatica, or other symptoms occur, a description of how the pain feels, and what activities, positions, or treatments make the pain feel better.
• Physical exam. The physician will conduct a thorough physical exam of the patient, such as testing nerve function and muscle strength in certain parts of the leg or arm, testing for pain in certain positions, and more. Usually, this series of physical tests will give the spine professional a good idea of the type of back or neck problem the patient is experiencing.
• Diagnostic tests. After the physician has a good idea of the source of the patient’s pain, a diagnostic test, such as an X-ray or MRI, is often ordered to confirm the presence of an anatomical lesion in the spine. The tests can give a detailed picture of the problem, such as the location of the herniated disc and impinged nerve roots.
Dr. Alan Dyer, the inventor of Vax-D, initially started the patient in a prone position. Working with Dr. Norman Shealy later and understanding the Nachemson study, they changed to a prone position.
You are lying face up. The automatic support system helps stabilize your upper body. The advanced computer system automatically adjusts to the proper angle of distraction. A lordotic air bladder system acts as a fulcrum to the angle of pull, allowing us to target specific discs causing your pain and symptoms.
The distractive forces utilize an algorithmic or sinusoidal curve to avoid proprioceptor response, which would create muscle spasm. The split table design decreases friction and allows separation of the vertebra, minimizing the effect of gravity.
Basically, you lie face up, and the computer works to keep your body comfortable. The effect on your back helps herniated material return to its normal position and stops the pain. Patients often describe the treatment as a gentle, painless, intermittent pulling of their back, and it can be so relaxing that many actually fall asleep during treatment.
Working with Life University, we will continue to provide ongoing articles and research. We are excited about the university’s certification programs, where you can also get hours of education. Go to the chiroevent. com. We look forward to seeing you in Florida to learn more about spinal decompression.

Dr. Eric Kaplan and Dr. Perry Bard, are business partners of over 32 years. They have developed Disc Centers of America & Concierge Coaches, now in the eleventh year, as well as the first and largest National Certification Program for Non-Surgical Spinal Decom pression. Currently, they have over 150 clinics using their Disc Centers of America brand and lead ongoing success training events throughout the year. For more information on coaching, spinal decompression, or seminars, visit www.TheChiroEvent.com or www. DecompressionCerti-fied.org or call the Chiropractic Q&A Hotline at 888-990-9660.

Dr. Jason Kaplan is a graduate of PARKER University. Along with his wife Dr. Stephanie Kaplan, they practice in Wellington Florida. Jason is an Instructor for Disc Centers of America. He has been recognized and honored by the International Disc Education Association and serves on the Medical Advisory Board for Non-Surgical Spinal Decompression. He teaches technique at the National Certification Program at Life University and is considered a Master on Non Surgical Spinal Decompression. www.WellinqtonDisccenter.com.

Dr. Devin Bard is an Adjunct Faculty to LIFE University. An author of the University Edition of the Ultimate Spinal Decompression Book. He opened one of the FASTEST Growing Record Setting DISC Centers of America Practices in the Country. His email is: [email protected].
References
1. Teraguchi M, Yim R, Cheung JP, Samartzis D. The association of high-intensity zones on MRI and low back pain: a systematic review. Scoliosis Spinal Disord. 2018 Oct 20:13:22. doi: 10.1186/sl3013-0180168-9. PMID: 30377668; PMCID: PMC6195950.
2. Namboothiri S, Gore S, Veerasekhar G. Treatment of low back pain by treating the annular high intensity zone (HIZ) lesions using rercutaneous transforaminal endoscopic disc surgery. Int J Spine Surg. 2018 Aug 15;12(3):388-392. doi: 10.14444/5045. PMID: 30276096; PMCID: PMC6159697.
3. Shahraki NM, Fatemi A, Agarwal A, Goel VK. Prediction of clinically relevant initiation and progression of tears within annulus fibrosus. J Orthop Res. 2017 Jan;35(l):113-122. doi: 10.1002/jor.23346. Epub 2016 Jul 8. PMID: 27325391.
4. Simon J, McAuliffe M, Shamim F, Vuong N, Tahaei A. Discogenic low back pain. PhvsMedRehabil Clin NAm. 2014 May;25(2):305-17. doi: 10.1016/j.pmr.2014.01.006. Epub 2014 Feb 28. PMID: 24787335.
5. Camp CL, Conti MS, Sgroi T, Cammisa FP, Dines JS. Epidemiology, treatment, and prevention of lumbar spine injuries in major league baseball players. Am J Orthop (Belle Mead, NJ). 2016 Mar-Apr;45(3): 137-43. PMID: 26991566.
6. Stadnik TW, Lee RR Coen HL, Neirynck EC, Buisseret TS, Osteaux MJ. Annular tears and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology. 1998 Jan;206(l):49-55. doi: 10.1148/radiology.206.1.9423651. PMID: 9423651.
7. Suthar P, Patel R, Mehta C, Patel N. MRI evaluation of lumbar disc degenerative disease. J Clin Diagn Res. 2015 Apr;9(4):TC04-9. doi: 10.7860/JCDR/2015/11927.5761. Epub 2015 Apr 1. PMID: 26023617; PMCID: PMC4437133.