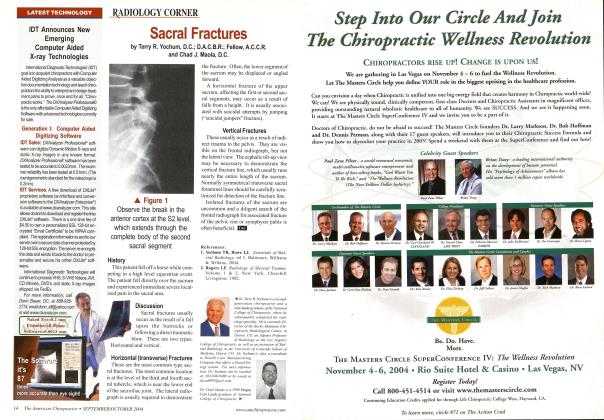
CASE HISTORY This adult male patient complains of back pain, especially at night, and it awakens him from sleeping. DISCUSSION Pedicle. The pedicle is an important radiologically detectable site for osteolytic mctastatic carcinoma. Any component of the neural arch can be involved, although the pedicle is by far the most common location. Destruction of the posterior vertebral body with contiguous involvement of the pedicle attachment results in loss of the cortical outline of the pedicle.1 This has been referred to as the one-eved pedicle sign or the winking owl sign and is most commonly found in the lower thoracic and lumbar spine. It is most easily visualized on the AP radiograph. Most cases of pedicle destruction involve a single vertebra; however, multiple levels can be affected. Occasionally, bilateral pedicular destruction may occur and is referred to as the blind vertebra. (Table 1) The most common cause for a missing pedicle is osteolytic metastatic carcinoma; however, agenesis of a pedicle may also occur. The key to radiologic differentiation is to search for a stress-related reactive sclerosis and enlargement of the contralateral pedicle. If this sign is present, it represents a firm assurance that osteolytic metastatic carcinoma is not present. Those cases of agenesis of the pedicle that create no stress hypertrophy of the opposite pedicle must be considered metastatic tumors until proven otherwise. Previous radiographs in this circumstance will be very helpful. Destruction of a pedicle in a patient under the age of thirty years is most commonly due to aneurysmal bone cyst (ABC), osteoblastoma, neurofibroma, or other cord tumors. Dr. Teny R. Yochum is a second generation chiropractor and a Cum Laudc Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology' tit the University of Colorado School of Medicine, Denver. CO. Dr. Yochum can he reached at 1-303-940-9400 or by e-mail at [email protected]. Dr. ChaclJ. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 1-303-690-8503 or e-mail DC_0 [email protected] Reference 1. Yochum TR, Rowc LJ: The Essentials of Skeletal Radiology, 3rd ed., Baltimore, Williams & Wilkins, 2005.1 Table 1. Radiologic Features of Spinal Metastasis LOCATION Lumbar/thoracic spine Vertebral body, pedicles SIGNS Altered bone density Decreased: moth-eaten, permeative diffuse Increased: localized, ivory vertebra Cortical destruction Disc space unaffected Pathologic collapse Decreased posterior vertebral body height Endplate disruption (malignant SchmorFs node) Pedicle destruction One-eyed pedicle sign (winking owl sign) Blind vertebra (both pedicles destroyed)